
Recommended EMS fluid resuscitation of burned casualties
(The casualties didn’t lose red blood cells, they lost volume: the liquid from their circulating volume has gone to their edema. The burns take fluid out of the vascular system and it needs to be replaced).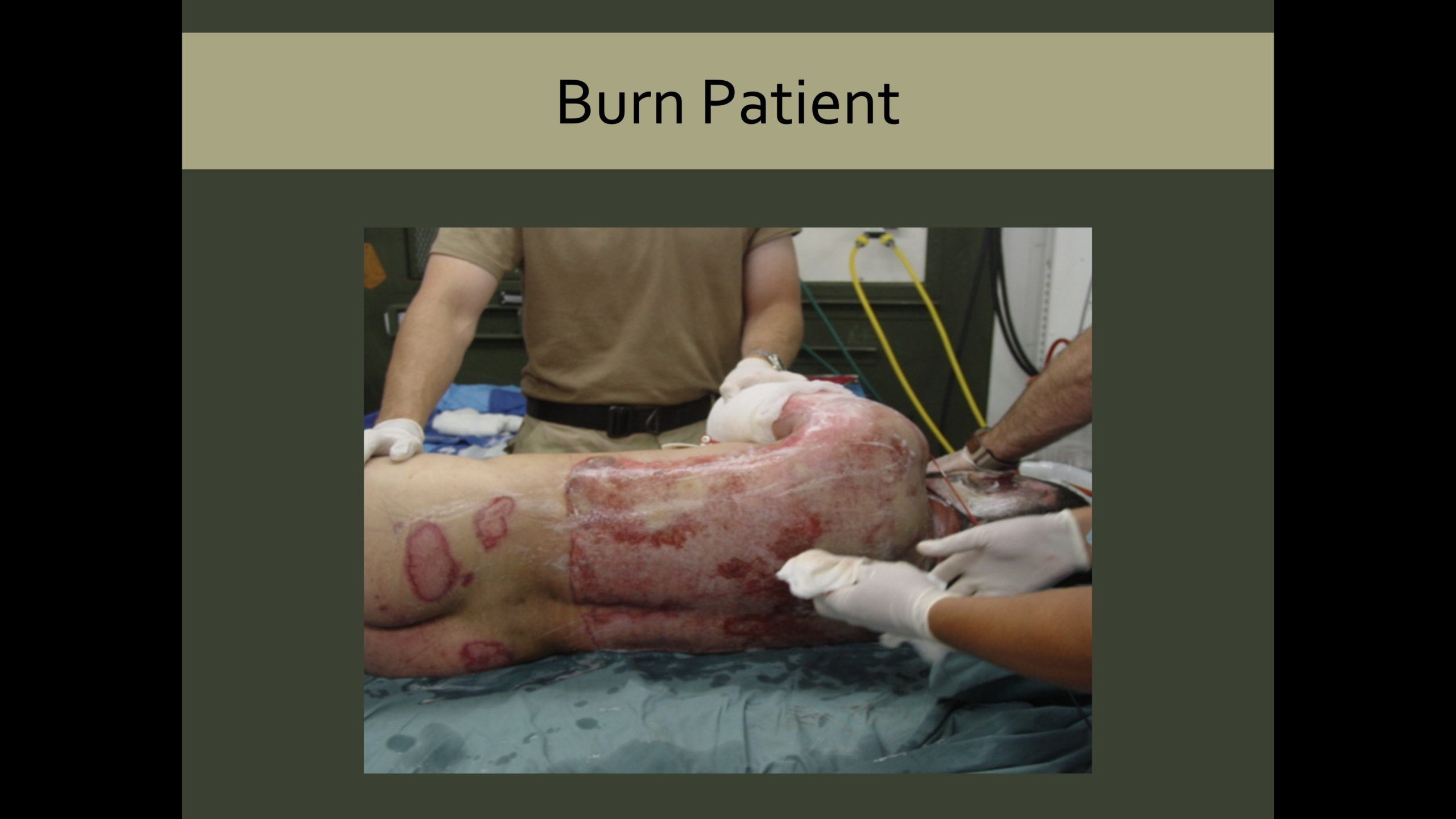
Although there are many formulas for fluid administration in burn casualties, the American Burn Association currently favors an initial set infusion of 500 ml LR per hour during the adult (14 years old or older) casualty’s initial evaluation. Once all life-threats have been treated, the patient stabilized, and TBSA determined, the Modified Brooke Formula is used for thermal burns. When calculating total body surface area burned, only partial and full-thickness burns are used. Superficial burns, such as akin to a sunburn, don’t count in the tabulation.



