
STAT Tourniquet: 21 of 24 applications FAIL
🕖 Reading Time, 6 minutes
Most recently, 84 volunteers with no prior tourniquet training applied either a STAT or 7th-generation CAT tourniquet to the HapMed leg trainer after viewing a 60-second manufacturer video on the device application. None of the STAT devices generated adequate hemorrhage control pressures. The average pressure generated by the volunteers was 409.9 mm Hg (CAT) versus 116.5 (STAT) with 57% of STAT applications less than 100 mm Hg pressure.1
UPDATE 2021: A subsequent study was completed and published in the American Journal of Emergency Medicine, their results mirrored ours. “In our pilot study, the CAT demonstrates significantly greater arterial occlusion pressures compared to the STAT in application on a lower limb hemorrhage model. This suggests the need for a larger scale investigation.”2
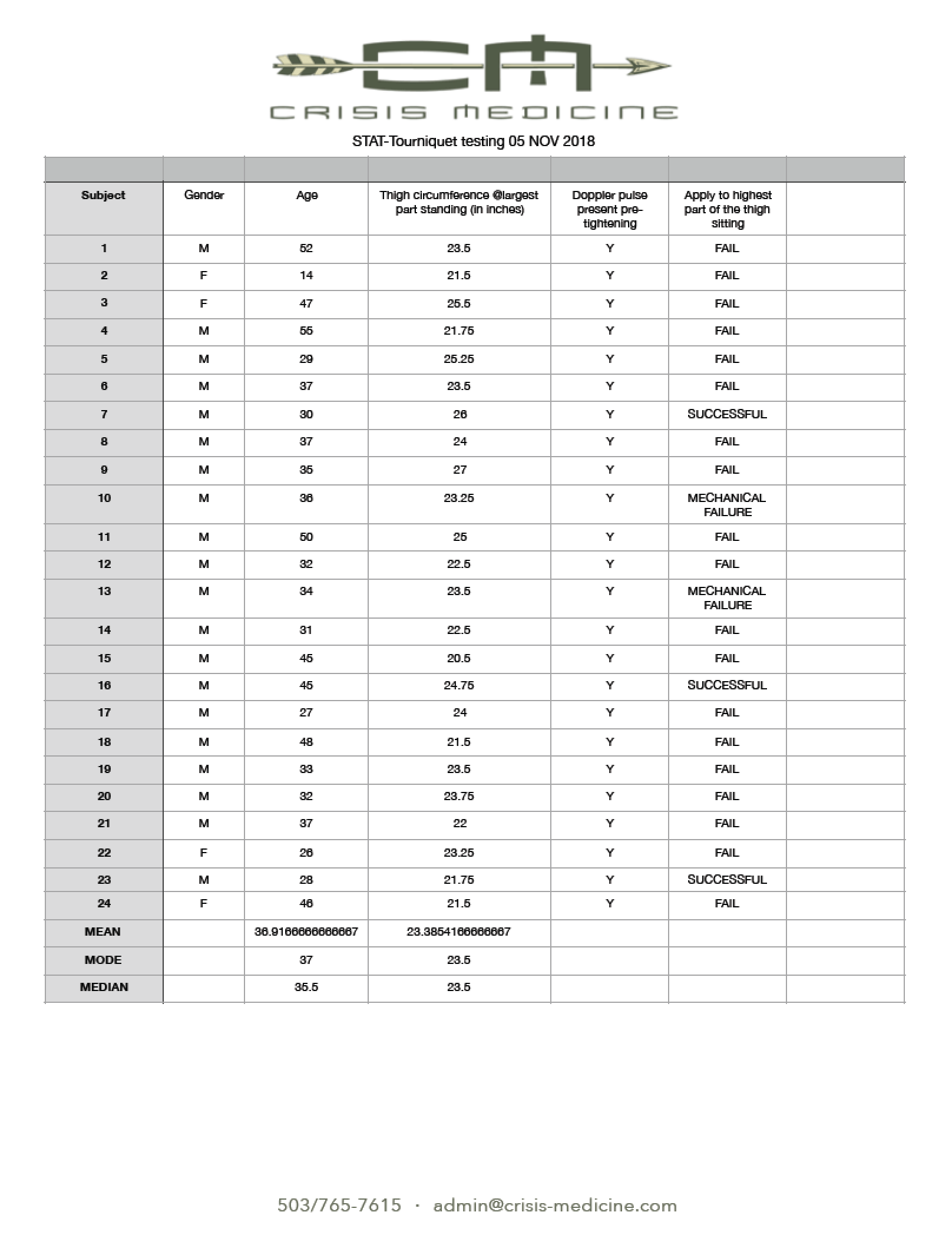
BLUF: We tested 24 self-applied high on the thigh STAT tourniquets on volunteers, verifying occlusion of arterial vascular flow by doppler ultrasound in the posterior tibial artery. We had 3 successful applications, 2 devices had mechanical failure (the locking mechanism slipped and would not allow continued tightening). Of the tested devices, 21 failed to achieve vascular occlusion.
STAT Medical devices is marketing a ‘new STAT tourniquet’ on social media, advertising it as a “mass casualty tourniquet.” After repeated questions from my law enforcement and fire colleagues about this device, I contacted STAT Medical on several occasions requesting information or medical literature demonstrating their product’s efficacy. I received no response.
Subsequently, we performed our own testing on the STAT tourniquet.
 A convenience sample of 24 firefighters and EMS related individuals was used to test the ability of 24 new STAT tourniquets to occlude femoral artery flow on doppler ultrasound. Tourniquets were purchased directly from the manufacturer at a cost of $474.75 for 25 tourniquets.
A convenience sample of 24 firefighters and EMS related individuals was used to test the ability of 24 new STAT tourniquets to occlude femoral artery flow on doppler ultrasound. Tourniquets were purchased directly from the manufacturer at a cost of $474.75 for 25 tourniquets.
Ages ranged from 14 (my daughter) to a 55-year-old firefighter/paramedic, comprising 4 females and 20 males. Standing thigh sizes were determined by placing the STAT tourniquet snugly around the largest part of the thigh, over their standard duty uniforms, marked, and then measured with a tape measure at the completion of testing. This technique likely overestimates thigh circumference somewhat. Accurate but not precise thigh measurements ranged from 20.5 inches to 27 inches. All of the testers have extensive experience self-applying CAT-tourniquets in training (yes, including my daughter).
Before tightening the STAT tourniquet, each tester was seated on the ground and asked to place the tourniquet as high on the thigh as possible. Their posterior tibial pulse was established with an 8.0 MHz Doppler ultrasound. Doppler pulsations were audible to the tester, who was then asked to tighten the STAT tourniquet until audible pulsation ceased or they were not physically capable of tightening it anymore. It was considered a device failure if audible pulsations could not be eliminated. If the device could not be maximally tightened because the locking mechanism repeatedly “slipped,” this was deemed a mechanical failure. Testers were allowed to use both hands to apply the device and try as many times as they desired. Each tester applied the device in a group setting, which provided a competitive environment. One tester commented, “I hope I’m successful so I can rub it in all day on you.”
We chose a high and tight tourniquet placement because it tends to be the most challenging location to achieve vascular occlusion. Advertising materials from the device manufacturer suggest a high and tight placement. This testing model and tourniquet application site was chosen because it is consistent with the evaluation of other commercially available tourniquets tested on human volunteers.
TRAIN NOWOnline Tactical Casualty Care Classes
Although the manufacturer recommends using a second device side by side if “bleeding doesn’t stop,” we chose not to do this in an attempt to evaluate the device consistent with the methodology of prior studies of commercially available tourniquets. Similarly, we chose to self-apply the tourniquets consistent with many of these studies. Unlike the USAISR “Navy Dive Study” in 2007, testers could hear the Doppler pulsation, which encouraged them to continue and try to tighten the tourniquet. 
NOTES:
1 Gabbitas RL, Carius BM. Smart Tactical Application Tourniquet Versus Combat Application Tourniquet: Comparing Layperson Applications for Arterial Occlusion After a Video Demonstration. Cureus. 2023 Jul 28;15(7):e42615. doi: 10.7759/cureus.42615. PMID: 37644942; PMCID: PMC10461781.
2Brandon M. Carius, Ashley D. Tapia, Nguvan Uhaa, Sarah A. Johnson, Camaren M. Cuenca, Ryann S. Lauby, Steven G. Schauer, STAT vs. CAT: A pilot comparison after a video demonstration, The American Journal of Emergency Medicine, Volume 47, 2021, Pages 305-306, ISSN 0735-6757, https://doi.org/10.1016/j.ajem.2021.01.017.
(https://www.sciencedirect.com/science/article/pii/S0735675721000206)


